The Brain Scan That Lies

Depression cannot be diagnosed through a brain scan and the fact that we wish it could, says something uncomfortable about us
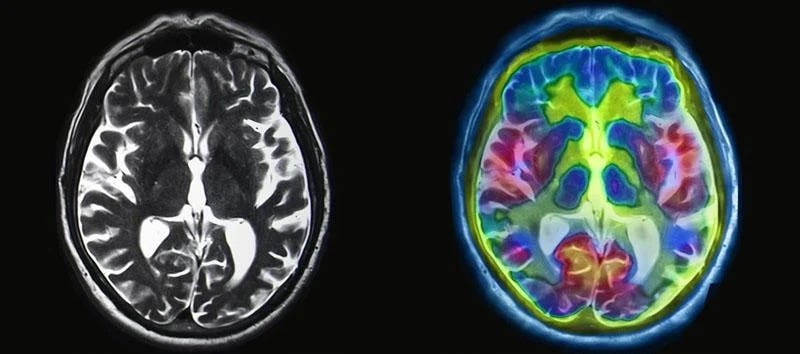
For years, psychiatry has flirted with the seduction of visibility. SPECT. fMRI. PET. Regions light up in red and yellow as though sadness could be heat-mapped like weather. The images feel authoritative. Once something is seen, it feels settled.
When psychiatrist Daniel Amen published SPECT scans of public figures - including Kim Kardashian - the scans looked cinematic, almost diagnostic in their confidence. Behavioral traits were inferred from blood-flow patterns. Dysregulation appeared circled in glowing colour.
The controversy focused on methodology. What fascinated me was the reaction.
If depression could be diagnosed from a brain scan, psychiatry would look very different.
Insurance companies would require imaging before prescribing SSRIs. Courts would demand scans in competency hearings. DSM criteria would include radiological markers.
None of that exists.
And yet millions of people have seen colourful brain images claiming to show ‘the depressed brain.’
Here is the uncomfortable truth:
Those same patterns can appear in people who are not depressed, and many people who are clinically depressed show scans that look entirely unremarkable.
That is not scandal. It is statistics.
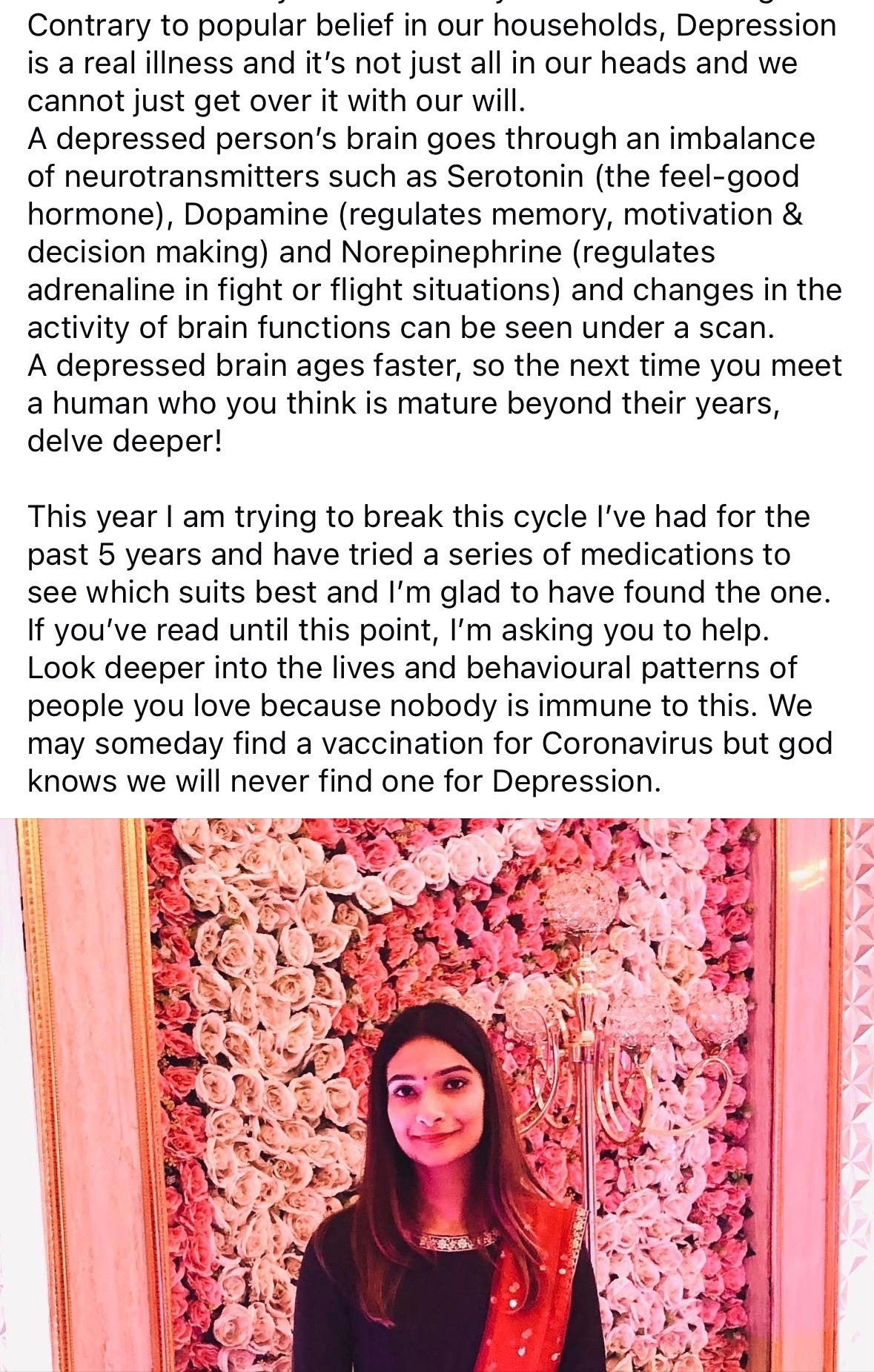
In 2020, I wrote about depression and neuroimaging. I wasn’t trying to provoke anything. I simply explained my experience of being depressed. The response surprised me. Messages poured in - not debating statistics, but expressing relief.
People told me they had no idea depression could “be seen” on a scan. Some said it made the illness feel real for the first time. Tangible. Medical. Valid.
One message said:
“I had no idea it could be seen in a scan, I’m so sorry you are going through this.”
That sentence stayed with me.
Because imaging does not measure despair. It does not quantify guilt, sadness, cognitive distortion, or suicidal ideation. SPECT measures regional cerebral blood flow. fMRI measures BOLD signal - oxygenation changes correlated with neural activity. These are indirect physiological proxies. Useful in research. Not equivalent to lived experience.
Large-scale collaborations like the ENIGMA Consortium have analysed thousands of scans, identifying statistically significant differences in cortical thickness and connectivity in major depressive disorder. Massive datasets such as the UK Biobank continue to refine associations between brain structure and mood phenotypes. Reviews in The Lancet Psychiatry and Nature Reviews Neuroscience consistently describe distributed network alterations - particularly within fronto-limbic and default mode networks.
The science is real.
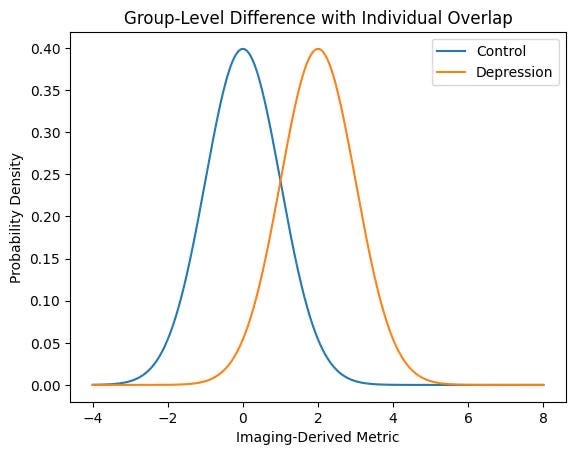
But it operates at the level of averages.
Group-level statistical significance does not equal individual-level diagnostic accuracy. Effect sizes remain modest. Overlap between depressed and non-depressed populations is substantial. Consensus analyses published in JAMA Psychiatry and the American Journal of Psychiatry are clear: no neuroimaging modality currently meets the sensitivity and specificity required for routine clinical diagnosis of depression.
If brain scans could diagnose depression, they would already be standard of care.
They are not.
The deeper issue is philosophical. We equate biology with visibility. If something is biological, we assume it must be photographable.
But depression is not a tumor. It is not a stroke. It is a systems-level dysregulation emerging from genetic vulnerability, inflammatory signaling, stress circuitry sensitization, developmental history, and lived narrative. Imaging captures one physiological slice of that complexity.
And yet I understand the hunger for proof.
When someone has been told to “snap out of it,” a scan feels like vindication. An image feels objective. A story can be dismissed as weakness; a coloured cortex cannot.
But scientific legitimacy is not granted by aesthetic authority.
In cardiology, troponin predicts myocardial injury. In endocrinology, HbA1c tracks glycemic burden. These markers alter decisions in real time. Psychiatric imaging - despite decades of refinement and increasingly sophisticated machine-learning models - has not reached that level of predictive utility.
Overstating its power does not help patients.
It replaces nuance with spectacle.
Brain scans are extraordinary research tools. They are reshaping models of mood regulation and network dysfunction. They may one day contribute to precision psychiatry.
But today, they cannot diagnose depression.
And mistaking visibility for validity may be one of the most expensive cognitive errors modern psychiatry continues to make.